Checklist 21 provides a guide for objective and subjective data collection in a musculoskeletal assessment
Checklist 21: Musculoskeletal Assessment
Figure 2.26 Muscular system
Figure 2.27 Skeletal system
Disclaimer: Always review and follow your agency policies and guidelines regarding this specific skill.
Safety considerations:
Perform hand hygiene.
Introduce yourself to patient.
Confirm patient ID using two patient identifiers (e.g., name and date of birth).
Explain process to patient.
Be organized and systematic in your assessment.
Use appropriate listening and questioning skills.
Listen and attend to patient cues.
Ensure patient’s privacy and dignity.
Document according to agency guidelines
Objective Data
Consider the following observations.
Steps
Additional Information
Observe ability to maintain trunk in upright position, mobility, assistive devices, bruising, curvature or abnormalities of the spine, presence of casts, braces, or splints.
General ability to move one’s body and maintain upright position reveals information about muscle strength and need for assistance with mobility needs.
Assistive devices should be in safe working order. Observe the patient’s ability to use these safely. See Chapter 3.5 Assistive Devices.
Any need for assistance, including mobility aids, should be included in the plan of care.
Observe range of motion (ROM) of upper and lower extremities.
Limitations in ROM may suggest articular disease or injury.
CWMS (colour, warmth, movement, sensation) assessment encompasses many systems and is a quick way to rule out concern(s).
View Assessing Range of Motion and Strength by Candace Walker and Wendy McKenzie Thompson Rivers University.
Inspect arms and legs for pain, deformity, edema, pressure areas, and bruises.
Unexpected findings should be followed with more detailed history and assessment, and reported to the appropriate healthcare provider.
Compare limbs bilaterally.
Assess motor power through hand grips, dorsi and plantar flexion, and knee and hip flexion against resistance.
General arm and hand strength can be assessed by asking the patient to extend their arms and grip the nurse’s hands simultaneously.
Apply slight resistance to top surface and ask patient to push against resistance.
Apply slight resistance to bottom of arms and ask patient to push against resistance.
Repeat with other arm
Figure 2.28 Assessing arm strength using resistanceFigure 2.29 Assess leg strength using resistance
Asymmetrical findings may suggest underlying conditions, injury, effects of some medications, or post surgical complications.
General leg strength can be assessed by asking the patient to dorsiflex while the nurse applies some resistance to the bottom of the feet. Plantar flexion strength can be assessed by asking the patient to pull-up on their feet while the nurse applies some resistance to the top of the feet. Have the patient elevate one leg to 30 degrees and hold. Apply slight resistance to top surface and ask patient to push against resistance. Apply resistance to the bottom surface and ask the patient to push against resistance. Repeat with other leg.
Figure 2.30 assess strength of dorsi flexion
Figure 2.31 Assess leg strength against resistance
Palpate limbs for abnormality.
Signs and symptoms of DVT include unilateral edema, pain, redness, and warmth at the site.
Any abnormalities or concerns should be reported to the appropriate healthcare provider.
Subjective Data
Ask about pain function, activity levels, joint problems, medications, and previous injury to extremities that may influence assessment findings.
Focused musculoskeletal assessment may include:
Determine Weight Bearing Status
Check orders for weight bearing status if applicable. Some surgeries require the patient to be non- or partial weight bearing afterward to optimize healing.
For example: non-weight bearing, partial weight bearing, feather weight bearing.
Falls Risk Assessment: Falls occur as a result of losing balance or inability to regain balance. A number of risk factors can be considered when predicting risk some of which are not modifiable (age) and others modifiable (diet, exercise, poor vision). Risk assessment tools help healthcare providers to predict risk and are the starting point of implementing strategies to reduce risk as much as possible.
Falls risk assessment is a routine part of nursing care in residential and acute settings. Communicate risk and appropriate interventions with the healthcare team and according to agency guidelines.
See:
Sample Motor Assessment Associated with Epidural Analgesia
0
No motor block: No intervention required.
1
Able to flex knees, but weak
2
Able to flex ankles. Can not flex knees
3
Cannot move ankles or knees
Adapted from OLCHC, 2016
Follow your agency guideline for the specific motor strength assessment scale used at your facility.
Potential nursing diagnoses:
Deconditioning related to immobility
Risk of falls
Altered mobility
Data Source: Assessment Skill Checklists, 2014; Jarvis et al., 2014; OLCH, 2016; Perry et al., 2018; Potter et al, 2019; Safer Health Care Now, 2015; Stephen et al., 2012; Wilson & Giddens, 2013
Potential musculoskeletal related nursing diagnoses:
Deconditioning related to immobility
Risk of falls
altered mobility due to
Data sources: Assessment Skill Checklists, 2014; Jarvis, Browne, MacDonald-Jenkins, & Luctkar-Flude, 2014; OLCHC, 2016; Perry et al., 2018; Potter, Potter, & Ostendorf, 2019; Safer Health Care Now, 2015; Stephen, Skillen, Day, & Jensen, 2012; Wilson & Giddens, 2013

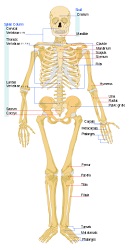


 Figure 2.30 assess strength of dorsi flexion
Figure 2.30 assess strength of dorsi flexion
